

Caution with immediate implant placement
Immediate implants are associated with greater variability in esthetic outcomes with a higher frequency of facial mucosal recession of >1 mm compared to early implant placement (Chen and Buser 2014; Hamilton et al. 2023). Careful assessment and analysis are crucial for appropriately determining any treatment plan, especially when proposing IIP treatment in the esthetic zone (Wittneben et al. 2023). An ethos of “minimizing morbidity without compromising long-term outcomes” should be prioritized.
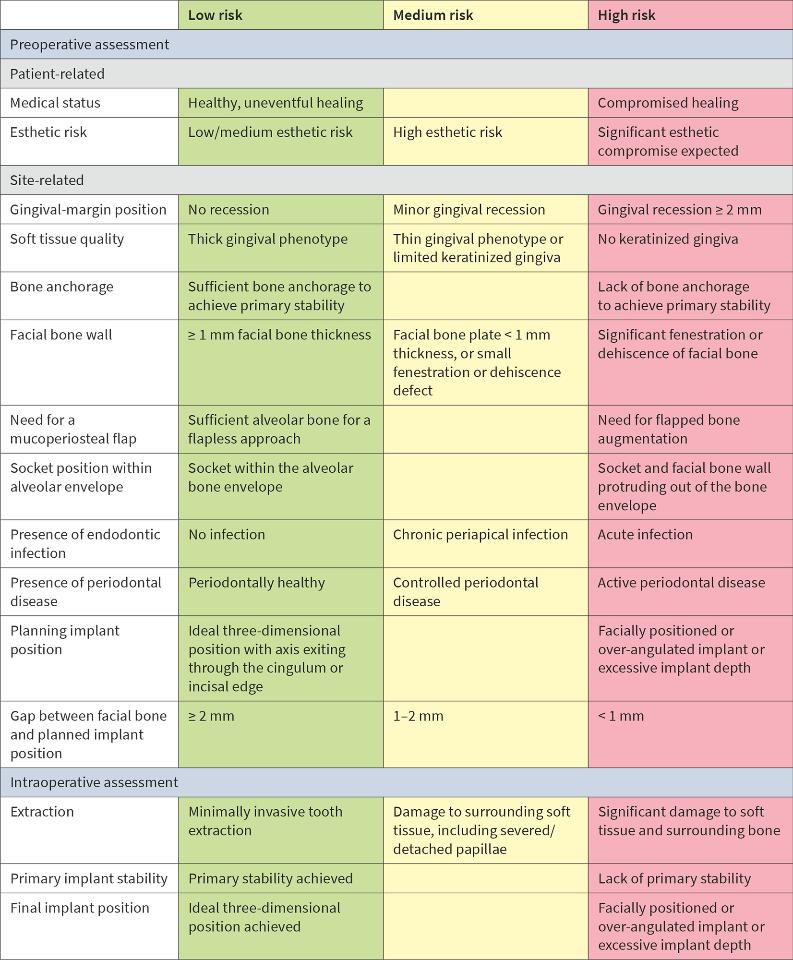
Patient and site-related factors must be considered for treatment to achieve predictable long-term functional and esthetic outcomes. The patient could be assessed using the Esthetic Risk Assessment (ERA) and risk assessment for IIP in single-tooth sites (Table 1) (Hamilton et al. 2023; Lambert et al. 2023) to determine the patient and site-specific risk factors for IIP. If the criteria for IIP protocol are not met, alternative placement protocols must be considered.
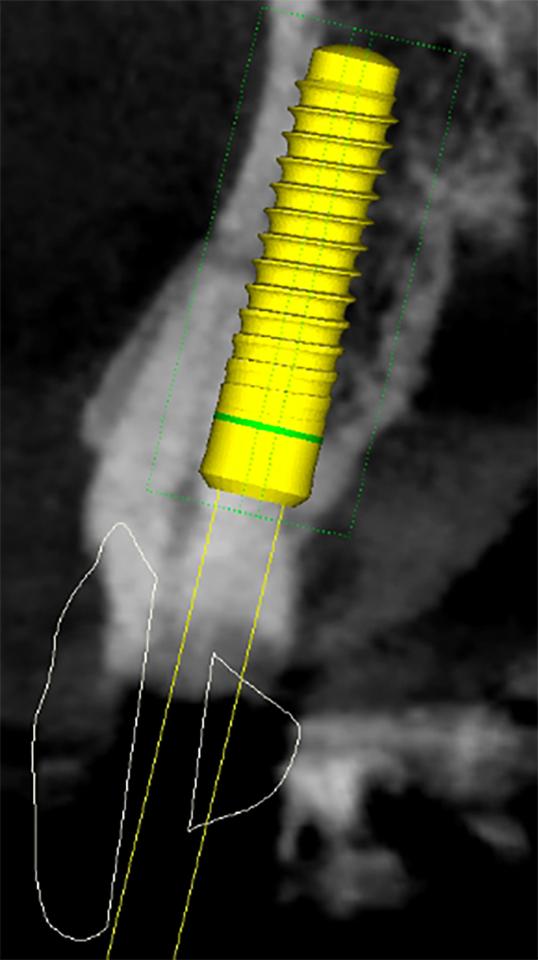
Optimizing esthetics for implant restorations in the anterior maxilla has been well studied, and implants should be restoratively driven irrespective of the timing of implant placement. It is critical to achieve an optimal, prosthetically-driven, three-dimensional implant position (Buser et al. 2004; Buser et al. 2017). In the anterior maxilla, midfacial recession has been reported for immediately placed BL implants in the presence of a thin (<1 mm) or missing facial bone plate (Chen et al. 2007; Seyssens et al. 2020). Further, clinical studies using CBCT scans to examine the facial bone on immediately placed implants have shown a significant relationship between recessions of the midfacial mucosa and a lack of visible facial bone on the CBCT images (Januário et al. 2011; Miyamoto & Obama 2011; Benic et al. 2012). The risks can be similar for TL implants, but the authors have experienced minimal risk of increased mucosal recession after placing TL implants in patients with <1 mm facial bone (Fig. 2). Although not currently supported by evidence, we attribute this to the simultaneous osseo- and mucosal integration that allows for better soft and hard tissue stability. Nevertheless, in some cases, loss of alveolar convexity has been noted, and the CBCT scans have confirmed the loss of alveolar convexity (Fig. 3).


After minimally traumatic extraction and preservation of facial bone plate, an immediate TL implant (NNC design) was placed (Type 1B) with simultaneous bone grafting in a 71-year-old male. The definitive restoration was placed 6 weeks later (Fig. 2c). For up to four years, the peri-implant tissues were stable with minimal recession, whilst there was a noticeable recession in adjoining natural teeth (Fig. 2d). There was minimal loss of alveolar contour despite <1 mm facial bone wall thickness (Fig. 2e). What is interesting to note here is that the bone is detectable coronal to the rough-smooth transition (Fig. 2f), which is not uncommon in our experience. Although histologically, this bone will not be “osseointegrated” with the machined collar, this thick, stable architecture achieved by the TL likely contributes to the long-term stable esthetics seen in our experience with TL implants.
In Figs 3a – c, a 75-year-old male requiring replacement of UL2 also has <1 mm facial bone thickness and pre-existing recession and a peri-apical lesion. Similar to the previous case, a Type 1B protocol with simultaneous GBR was chosen (Fig. 3d) (Gallucci et al. 2018). Loss of alveolar convexity was noted within weeks of provisionalization, even though the submarginal emergence of the crown was optimally shaped (Figs 3e – g). Nevertheless, the 1- and 2-year reviews show an excellent esthetic outcome (Figs 3h – k), which compares well with the pre-operative situation.
These two examples reiterate that outcomes with Type 1 protocols, especially the response of bundle bone resorption and its impact on bone graft particles, can be unpredictable, even with TL implants.
Interestingly, pre-clinical studies have consistently demonstrated that irrespective of implant type or dimension, resorption of bone after tooth extraction occurs (Araujo & Lindhe 2005; Caneva et al. 2010; Linares et al. 2011). Caneva and coworkers highlighted the need for sufficient space between the implant and the buccal bone. They studied the influence of the distance of the implant surface to the buccal bone for IIP by comparing 3.3-mm and 5-mm diameter implants. Marginal bone loss in wider diameter implants was more marked compared to the narrow diameter implants. This risk is heightened in thin phenotypes, so coronally tapered implants such as the Straumann TE are now not commonly used for IIP. Therefore, IIP in sites with a facial bone thickness of <1 mm should be considered a risk for loss of alveolar root convexity and midfacial recession. In such cases, if IIP is preferred, soft tissue augmentation at the time of placement should be considered (Seyssens et al. 2021).
One of the main concerns regarding TL in the esthetic zone is the risk of shine-through or exposure of the machined collar. In our experience, these complications result solely from surgical error and due to facial malpositioning of the implant (Chen et al. 2007; Chen et al. 2009), resulting in recession and esthetic failure (Chen & Buser 2009; Cosyn et al. 2019; Evans & Chen 2008). Most importantly, these complications arise irrespective of the chosen implant design.
Tissue level implants in the Type 1 immediate protocol should be placed, adhering to the principles of 3-dimensional implant placement (Figs 4 – 5):
Apico-coronal position: not more than 2-3 mm apical to the proposed mucosal margin,
- Oro-facial position: ideally screw-retained with screw access through the cingulum. A minimum of 2-mm horizontal gap should be maintained between implant and internal socket wall at the junction of the rough surface,
- Mesio-distal position: >1.5 mm distance from implant shoulder to adjacent teeth.